
- 12 Jun 2026
- Joseph Renny, Simon N. G. Tyler
From Undruggable to Inevitable: Fifteen years of drug development — and what comes next

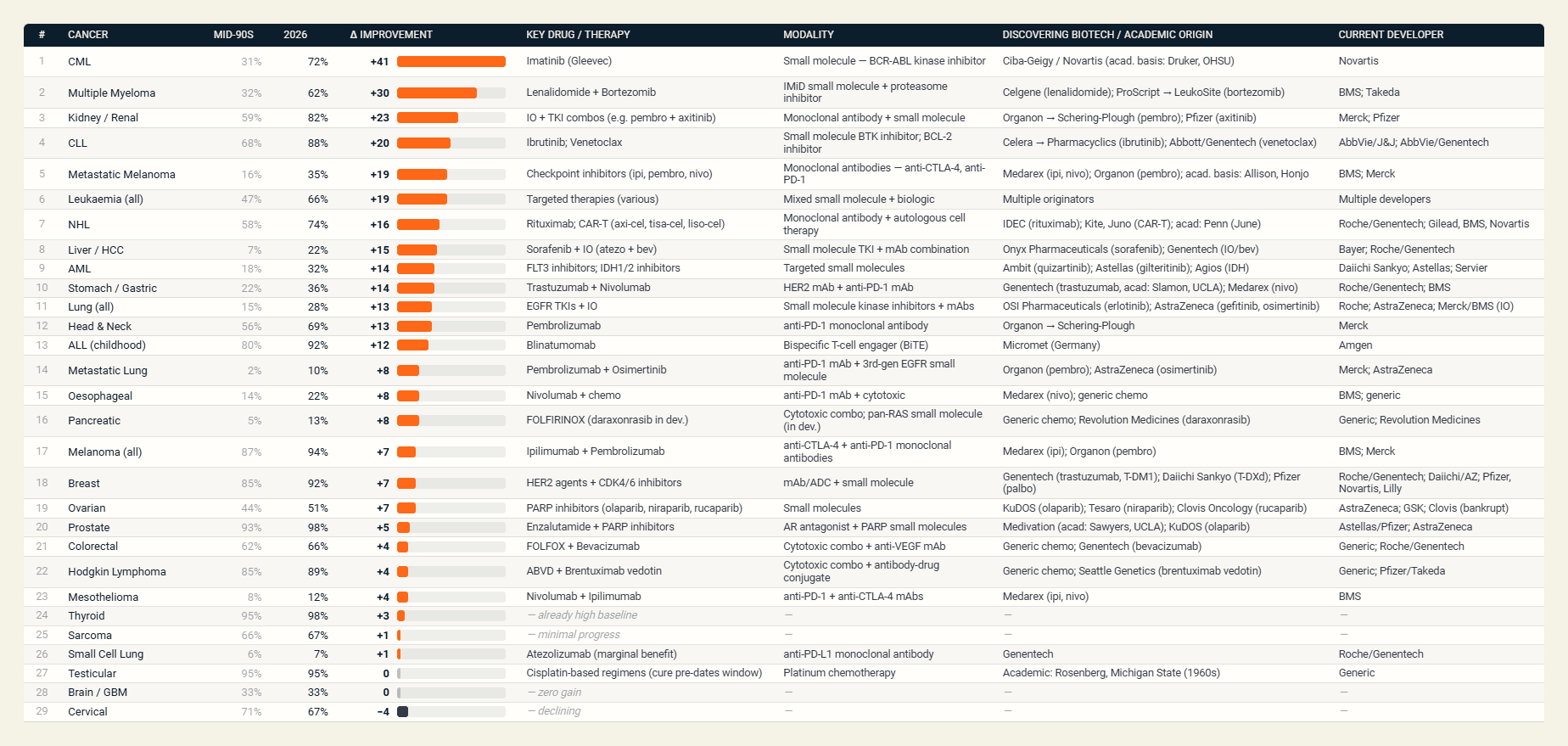
The American Cancer Society’s 2026 statistics tell a story that should be on the wall of every drug developer. Five-year survival for chronic myeloid leukaemia has risen from 31% in the mid-1990s to 72% — a forty-one-point gain credited largely to a single small molecule, imatinib. Multiple myeloma is up thirty points; metastatic melanoma, once a near-certain death sentence, has more than doubled. Behind each of those gains sits a different kind of molecule, a different mechanism, a different manufacturing challenge — and, increasingly, a different way of finding the molecule. And cancer is only one slice of a wider transformation now spanning metabolism, infectious disease and the rarest inherited conditions.
Fifteen years ago, when CatSci was founded, the conversation was dominated by small-molecule kinase inhibitors and an emerging wave of monoclonal antibodies, and the mood was anxious: the first great patent cliff was approaching, pipelines were thinning, and the industry was restructuring on a scale not seen in a generation. CatSci itself was spun out of that moment — born of AstraZeneca’s exit from the Avlon Works at Avonmouth, where a generation of process chemistry expertise needed a new home — and the specialist enterprises that emerged across the industry would become part of the infrastructure on which the modern medicine ecosystem now rests. The science of the time, meanwhile, had served up a roll-call of targets pharmacologists couldn’t reach: KRAS, MYC, the tau protein, much of the transcriptional machinery. We called them undruggable then. That’s no longer the case for most of them.
The modality explosion
The most obvious shift since 2011 is that “the molecule” no longer means just a 500 Da, orally available, rule-of-five-compliant small molecule. It means whichever of a dozen modalities is best matched to the biology in front of us. Antibody-drug conjugates have moved from a single product to a portfolio; bispecifics like blinatumomab have lifted paediatric ALL survival past 90%; CAR-T, once a heroic last resort, is now mainstream in B-cell malignancies, and pushing into solid tumours and autoimmune disease. mRNA, vindicated by the COVID-19 pandemic, is being engineered into oncology vaccines and rare-disease and cardiometabolic indications. PROTACs and molecular glues are turning protein degradation into commercial reality, and small molecules themselves have been reborn — covalent inhibitors, allosteric binders and degraders unlocking surfaces of the proteome that were off-limits a decade ago.
KRAS is the symbolic conquest. For four decades, a smooth, featureless GTPase that drives roughly a quarter of human cancers sat on every undruggable list; by 2021 sotorasib had broken the seal, and pan-RAS inhibitors are now reshaping the outlook for some of the most stubborn cancers, pancreatic among them. But the lesson isn’t really about KRAS — it is that “undruggable” was always a description of our chemistry, not of biology. Each new modality redefines the target universe: PROTACs need only a surface and a ligase, not a deep pocket; oligonucleotides intervene upstream of the protein; mRNA supplies a missing protein rather than inhibiting one; cell therapies recognise targets rather than bind them. Each turns a class of impossible diseases into a class of programmes.
Beyond oncology, and beyond the patient
It is easy to read the leaderboard as a cancer story; it isn’t. The rise of GLP-1 receptor agonists — semaglutide, tirzepatide and the next generation in late-stage development — is the most consequential cardiometabolic story of the era. What began as a diabetes therapy has become a treatment for obesity, and through obesity for cardiovascular risk, sleep apnoea, fatty liver and kidney disease, reaching tens of millions of patients. The development challenge has been quieter but no less significant — these are complex peptides, made at a scale that has tested the global supply chain. Shortages in 2024 and 2025 reminded the industry that a successful medicine without manufacturing capacity is barely a medicine at all.
Infectious disease deserves its own place on the leaderboard. Hepatitis C — a chronic, ultimately fatal infection for millions — became curable almost overnight with the direct-acting antivirals, a small-molecule story to rank alongside imatinib. Yet the same field holds medicine’s starkest unmet need. Antimicrobial resistance is largely tractable scientifically but commercially challenging: an antibiotic that works is one society wants used as little as possible, which destroys the economics of developing it — a rare case where the market punishes success, and where new push-and-pull funding models are being trialled to keep a pipeline alive at all.
Rare and orphan disease tells a different but related story, and a morally important one. There are roughly seven thousand rare diseases, the great majority still without an approved therapy. Two technologies have changed that calculus. Antisense oligo and siRNA medicines now reach conditions untreatable a decade ago — nusinersen for spinal muscular atrophy, patisiran for hereditary amyloidosis — while gene therapy and editing have gone further: onasemnogene abeparvovec replaces a missing gene in infants with SMA, and exa-cel uses CRISPR to edit a patient’s own stem cells in sickle cell disease. Each would have been science fiction in 2011.
The moral weight here is not subtle: these are conditions affecting children and families with no alternative, and for the first time the science exists to help them. But although the impact does not stop at the individual patient, a one-time gene therapy with a multi-million-dollar list price front-loads a lifetime of cost into a single invoice — something the actuarial machinery of insurers and health systems was never built to handle, and which has forced new payment models: outcomes-based agreements, annuity-style instalments, shared risk pools. A GLP-1 priced modestly per patient becomes a budget problem precisely because it works for a population in the hundreds of millions. Both scenarios describe the same shift from chronic treatment that spreads cost predictably toward durable or population-scale interventions that concentrate value, and the bill. For payors, the question is increasingly not only whether a therapy works, but whether the system can afford the way it works — the art and science of health economics is booming: a reminder that delivering a breakthrough now demands innovation in financing and access as much as in chemistry.
The CMC frontier just got harder
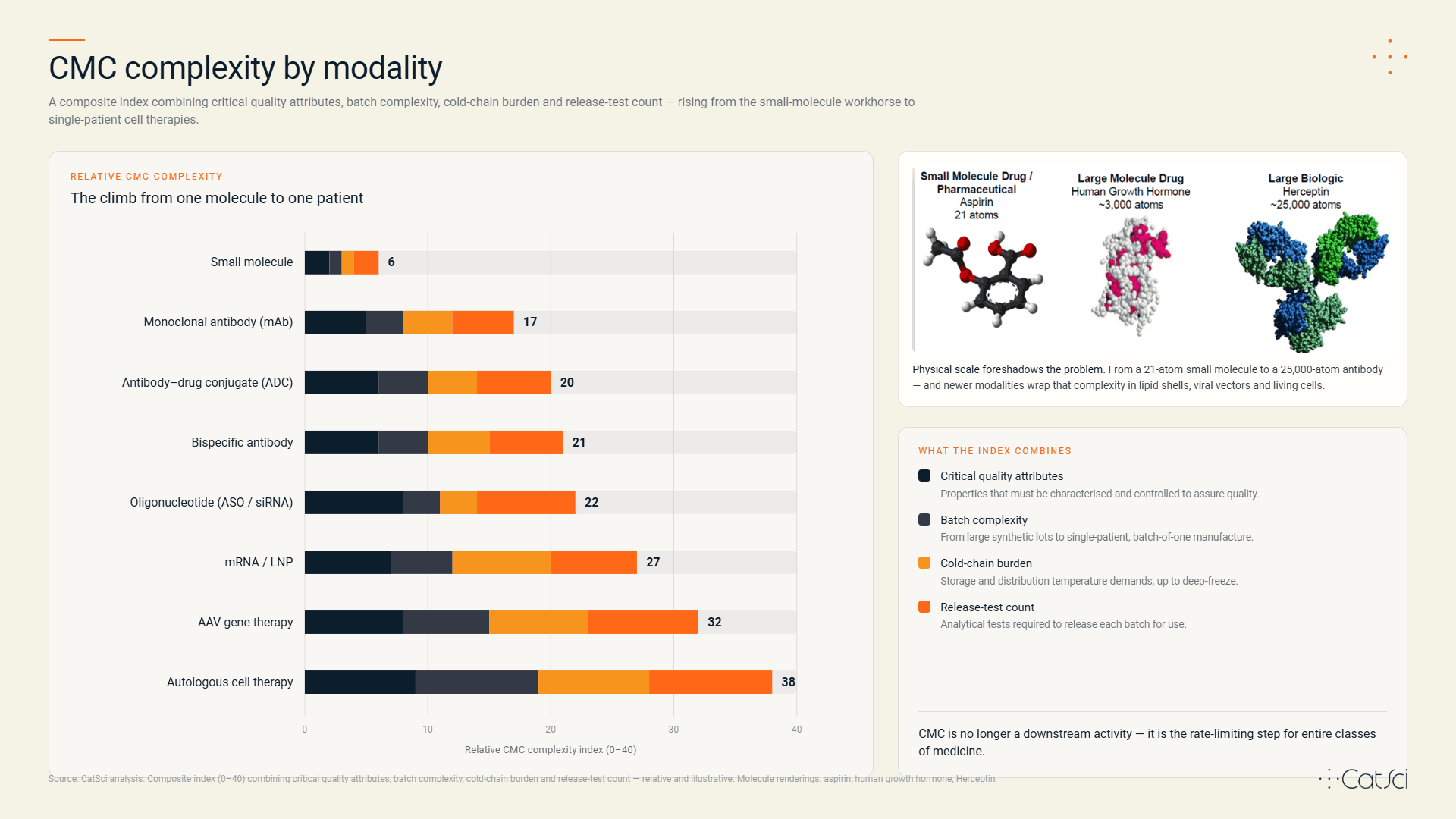
This proliferation of modalities is, from a drug developer’s seat, equal parts thrilling and humbling: each new format brings its own chemistry, manufacturing and controls (CMC) puzzle, and the puzzles do not get easier with scale. Small molecules remain the workhorse, but they have grown bigger and more three-dimensional — beyond-rule-of-five chemistry, macrocycles and covalent warheads make route design a matter of strategy, not just scale-up. ADCs ask teams to be excellent at three disciplines at once: payload synthesis, biologics manufacture, and conjugation chemistry characterised to a degree earlier biologics never required. mRNA and gene therapies brought lipid nanoparticle formulation, cold-chain logistics, and a dependence on plasmid and viral-vector supply chains that did not exist at industrial scale a decade ago. Protein degraders and molecular glues introduce ternary-complex assays and impurity profiles that are anything but conventional.
The shared theme is that process and analytical challenges scale super-linearly with modality complexity. A monoclonal antibody (mAb) may need around a hundred release tests; an autologous cell therapy can require many more, on a single-patient batch. CMC is no longer a downstream activity — it is the rate-limiting step for entire classes of medicine.
AI: from curiosity to co-pilot
The other fifteen-year arc is computational. In 2011, in silico drug design meant docking and QSAR. By 2026, it means foundation models trained on protein structure, generative chemistry that proposes synthesisable analogues, and retrosynthesis engines that recommend routes a human might not have considered.
AlphaFold and its successors did for structural biology in five years what crystallography did in fifty, and generative models alongside laboratory automation have changed the unit costs of medicinal chemistry: a programme that took five years and a hundred chemists in 2015 can now reach an IND-enabling candidate with a smaller team and in less time. AI is increasingly present in CMC too — solid-form properties, formulation prediction, process modelling amongst others. But the temptation is to overstate it. AI does not yet design a molecule, route, formulation and manufacturing process end-to-end; what it changes is the economics of trying, letting hypothesis-rich teams ask more “what if” questions, earlier. The teams who win the next decade will be those who integrate AI into their experimental discipline rather than bolt it on the side.
Innovation has changed its address
From where breakthrough medicines come has shifted almost as dramatically as what they are. In 2026 roughly two-thirds of novel FDA approvals originate from outside large pharma — in biotechs, academic spin-outs and publicly-funded consortia. Big pharma has not retreated; it has changed role: its advantage no longer the discovery bench, but rather the bench-to-bedside chain of late-stage development, global trials and manufacturing scale. The lineage of almost every modality runs back through an academic laboratory — checkpoint inhibition through Allison and Honjo, CRISPR through Charpentier and Doudna, mRNA through Karikó and Weissman’s years of rejected grants. The unprecedented insight comes from somewhere small; the medicine eventually emerges from a larger system putting capital and infrastructure around it. Biotechs that own a brilliant molecule rarely own the CMC expertise or facilities to take it from gram-scale to GMP — the CRDMO ecosystem exists to bridge that gap, and fifteen years on it is global, specialised and indispensable.
And the cycle is turning again. A second patent cliff is approaching — several of the biggest medicines of the last decade lose exclusivity within five years — and large companies are once more re-shaping their R&D and manufacturing footprints, as any well-run business does when its environment changes. As before, that restructuring is producing talent and capacity that finds new homes in biotech innovators and the specialist service providers on which those same companies increasingly rely. None of these players could deliver a modern medicine alone; the ecosystem itself is the asset. The more the industry changes, the more it stays the same.
The next fifteen years
If the past fifteen years were about expanding the toolkit, the next will be about convergence — ADCs with bispecific targeting, degraders delivered as mRNA, cell therapies with small molecule safety switches. Beyond that, three trends look durable. Manufacturing will move closer to the patient: point-of-care production of cell therapies, personalised vaccines and gene-editing payloads, already operational at small scale, will be ordinary within a decade — and as editing moves in vivo, the cell no longer has to leave the patient to be corrected, turning some gene therapies into something closer to a conventional injectable. CMC will embrace data science as deeply as it once absorbed statistics, with digital twins and continuous manufacture becoming the norm. And discovery and development will keep blurring — by the time a candidate reaches nomination, its synthesis, polymorph behaviour and even formulation will already have been substantially predicted in silico, the experimental laboratory evolving to confirm rather than discover.
None of this should be mistaken for a victory lap, however. The most prevalent diseases of the brain remain largely unconquered — the anti-amyloid antibodies now approved in Alzheimer’s deliver modest benefit at real cost and risk, and Parkinson’s, ALS and Huntington’s are still waiting for their imatinib. Antimicrobial resistance outruns the pipeline meant to counter it. And the geography of access remains starkly uneven: tuberculosis and malaria still kill at scale in the places least able to pay for the science that could prevent it. The honest reading of the leaderboard is that it shows what becomes remarkable possibilities can be realised when science, modality and economics align; the work that remains is to make that alignment the rule rather than the exception.
Still, the gains are real and they compound. Most of the molecules behind that progress did not exist when CatSci opened its doors; few resemble each other, and none were inevitable. They are the product of the last fifteen years of restless reinvention that itself stood on the shoulders of giants before. Of the molecules, the manufacturing, and the tools we use to discover and develop both. Of the partnerships across academia, biotech, big pharma and the CRDMO ecosystem that must co-operate to turn target into medicine. Breakthrough science for the benefit of patients knows no boundaries — institutional, geographic, commercial or therapeutic — and the proof now spans oncology, metabolism, infectious disease, neuroscience and rare disease alike.
If the last fifteen years taught us that ‘undruggable’ was a temporary description, the next fifteen will determine which diseases stay incurable only because we have not yet got round to them.